RESEARCH SPOTLIGHT
Local real‑world evidence on statin choice in diabetes: Choosing rosuvastatin for CV gains



In brief
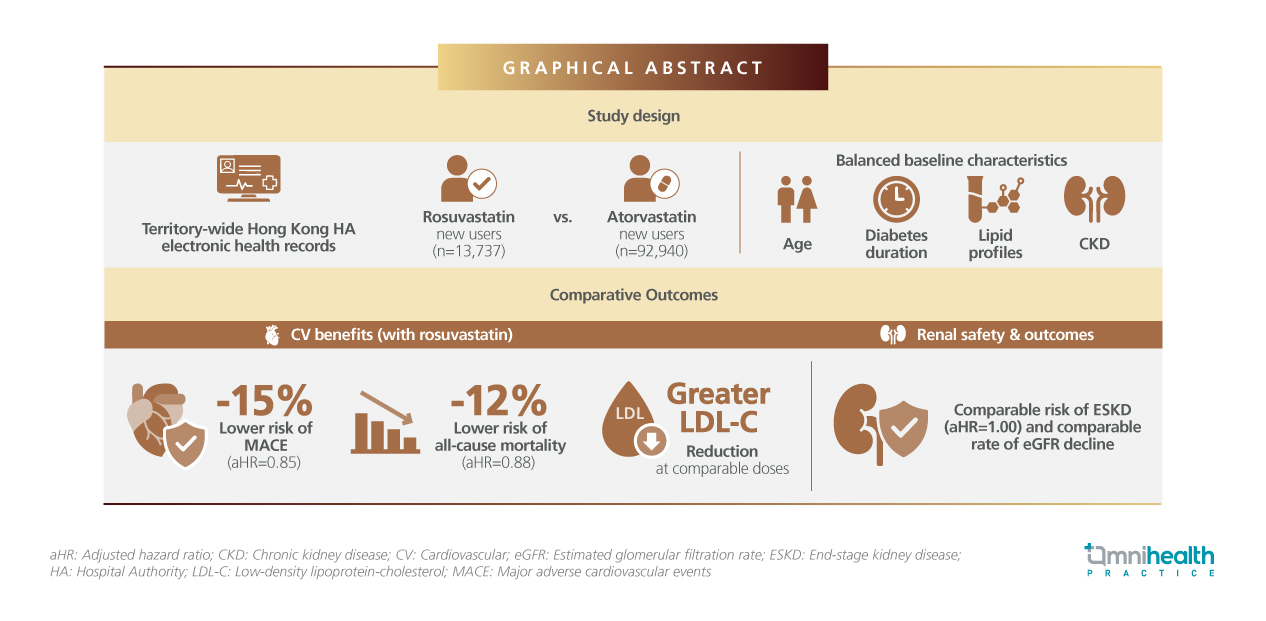
This study analyzed 106,677 Chinese patients with diabetes across chronic kidney disease (CKD) stages who received rosuvastatin (n=13,737) and atorvastatin (n=92,940) over a median follow‑up of 2.33 years.1 It was found that rosuvastatin and atorvastatin carried a comparable risk for the primary outcome of end‑stage kidney disease (ESKD) (adjusted hazard ratio [aHR]=1.00; 95% CI: 0.91‑1.11).1 Rosuvastatin provided superior cardiovascular (CV) benefits when accounting for real‑world treatment patterns over time, significantly lowering the risk of major adverse cardiovascular events (MACE) by 15% (HR=0.85; 95% CI: 0.77‑0.93) and all‑cause mortality by 12% (HR=0.88; 95% CI: 0.81‑0.96).1 Rosuvastatin also demonstrated superior potency in lowering low‑density lipoprotein (LDL) cholesterol (LDL‑C) levels compared to atorvastatin, a benefit that enables attainment of lipid goals at standard moderate‑intensity dosages.1
Background
Patients with diabetes in Hong Kong carry a substantial burden of atherosclerotic cardiovascular disease (ASCVD), driven by long disease duration, aging demographics, and a high prevalence of cardiometabolic comorbidities.1 CKD is common in this population and further amplifies CV risk, making effective lipid management a clinical priority.¹ Statins remain the cornerstone of CV prevention in patients with diabetes.¹ However, differences in LDL‑C‑lowering potency, dose requirements, and safety profiles may influence agent selection.1
Previous studies, such as the PLANET 1 trial, primarily focus on a white population and fail to account for the higher plasma exposure of rosuvastatin among East Asians.1 Rosuvastatin delivers greater LDL‑C reduction at moderate intensity doses.1 By leveraging territory‑wide Hong Kong Hospital Authority (HA) real‑world data, this study provides clinically relevant evidence on the CV and renal outcomes of rosuvastatin in a population highly representative of everyday Hong Kong practice.1
Methodology
This population‑based study utilized comprehensive real‑world data extracted directly from the HA electronic health record system.1 The study design was an emulated target trial.1 The final cohort was representative of the local clinical landscape, encompassing 106,677 Chinese patients (aged 18 years and older) diagnosed with diabetes between the years 2002 and 2019.1 Within this extensive cohort, researchers identified 92,940 patients who were initiated as new users of atorvastatin and 13,737 patients who were initiated as new users of rosuvastatin.¹ The baseline renal characteristics of the cohort were diverse, with 75.80% of patients classified at CKD stages G1‑G2, 20.47% at stage G3, and 3.72% at stage G4.1
To control for confounding by indication and ensure baseline characteristics were balanced between the two drug cohorts, the researchers applied a propensity‑score overlap‑weighting (PS‑OW) statistical approach.¹ This advanced weighting method successfully balanced all measured baseline covariates, including age, diabetes duration, lipid profiles, baseline estimated glomerular filtration rate (eGFR), and pre‑existing comorbidities, yielding a highly comparable pseudo‑population.¹
The primary renal outcome investigated was the incidence of ESKD, which was strictly defined as the initiation of dialysis, kidney replacement therapy, or a sustained eGFR of less than 15mL/min/1.73m².¹ Secondary clinical endpoints included MACE, defined as a composite of non‑fatal myocardial infarction, non‑fatal stroke, and CV death, as well as all‑cause mortality.1 Additional critical kidney endpoints measured over the follow‑up period included the onset of new albuminuria and the annual eGFR slope, which tracks the rate of kidney function decline.¹ To reflect real‑world clinical practice, where patients frequently adjust, switch, or discontinue medications, the researchers employed a sophisticated time‑varying Cox proportional hazards model to calculate the hazard ratios (HRs) for these outcomes.¹
Results
Rosuvastatin achieved greater LDL‑C reduction than atorvastatin at comparable statin intensities, with the difference being most apparent at the moderate doses.¹ Specifically, moderate‑intensity rosuvastatin (5‑10mg/day) provided stronger LDL‑C lowering than moderate‑intensity atorvastatin (10‑20mg/day), enabling more LDL‑C lowering within the same dose range.² Beyond these advantages in lipid control, this higher potency translates into significant, long‑term renal, CV, and survival benefits (table 1).1
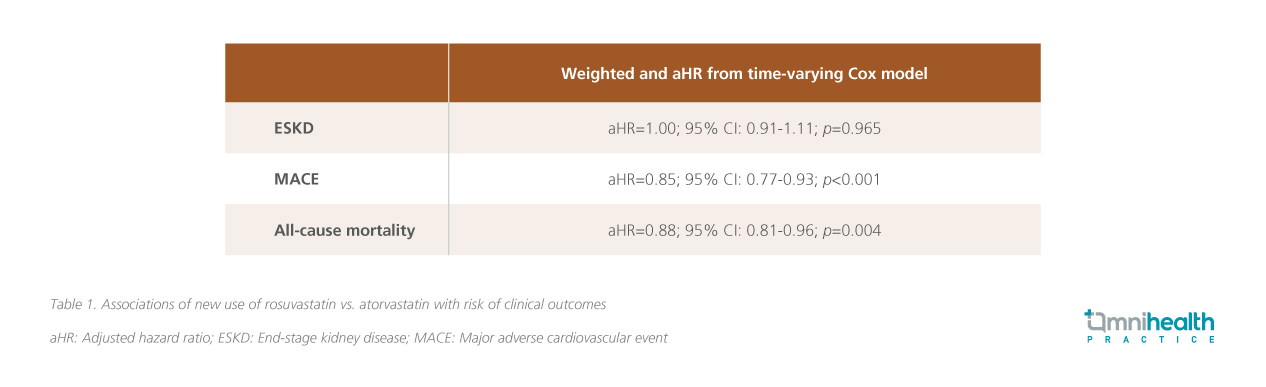
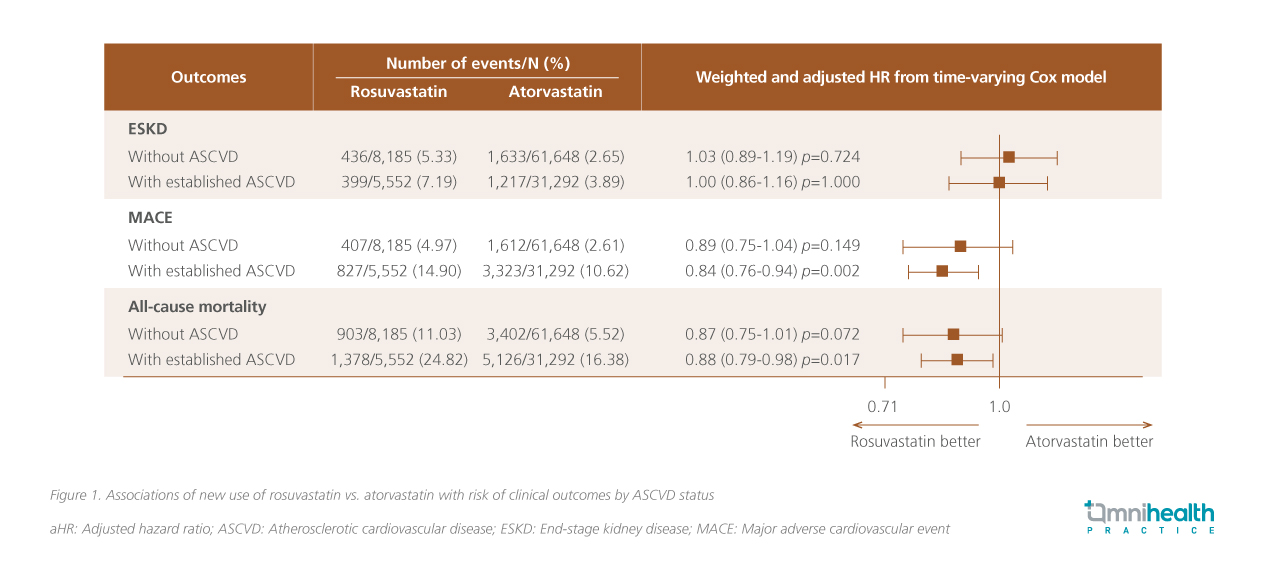
Rosuvastatin use was associated with a 15% lower risk of MACE compared with atorvastatin (HR=0.85; 95% CI: 0.77‑0.93).¹ This reduction in CV events was observed when treatment exposure was analyzed dynamically, reflecting real‑world patterns of dose adjustments, switching, and discontinuation.¹ This suggests that rosuvastatin's CV benefits are maintained over time.¹ In addition to reducing CV events, rosuvastatin was associated with a 12% reduction in all‑cause mortality (HR=0.88; 95% CI: 0.81‑0.96).¹ This mortality benefit provides vital reassurance for patients with diabetes and CKD, where non‑CV causes of death contribute substantially to overall risk, reinforcing rosuvastatin as an option that delivers benefits extending beyond lipid control.¹ While the rosuvastatin offers risk reduction in CV and mortality outcomes, it is also important to weigh these benefits against its specific renal safety profile. The risk of progression to ESKD was similar between the two treatments (HR=1.00; 95% CI: 0.91‑1.11), indicating no excess long‑term renal failure risk associated with rosuvastatin use.¹ Notably, these effects were seen across baseline ASCVD status (figure 1).¹
This neutral outcome provides important clarity, given historical concerns regarding rosuvastatin's renal effects extrapolated from Western datasets.¹ The annual decline in eGFR was nearly identical between treatment groups (‑1.73mL/min/1.73m² per year for rosuvastatin vs. ‑1.74mL/min/1.73m² per year for atorvastatin, p=0.905).1 Over time, rosuvastatin does not accelerate the loss of kidney function relative to atorvastatin, even in patients with underlying CKD.¹ However, new‑onset albuminuria occurred more frequently with rosuvastatin (HR=1.30; 95% CI: 1.16‑1.47), with the risk increasing at higher doses.¹ The dose‑dependent nature of this finding supports a clinical strategy of appropriate dose selection and routine urinary albumin monitoring rather than avoiding rosuvastatin entirely.¹ Importantly, this albuminuria signal was not accompanied by increased ESKD risk or faster eGFR decline.1
Discussion
Rosuvastatin provides clinically meaningful CV advantages for patients with diabetes in Hong Kong, a population inherently characterized by high baseline CV risk.¹ Crucially, this benefit extends to patients with coexisting CKD, a demographic traditionally considered challenging to manage due to overlapping CV and renal risks.¹ The observed reductions in MACE and all‑cause mortality demonstrate that rosuvastatin delivers benefits extending beyond mere lipid lowering, translating biochemical efficacy into tangible survival advantages.¹
While rosuvastatin offers CV and survival advantages, the drug's specific renal safety profile should also be considered.1 Despite historical concerns regarding rosuvastatin's potential renal effects, long‑term kidney outcomes in this study, including progression to ESKD and the trajectory of eGFR decline, were comparable to atorvastatin.¹ The absence of excess risk for irreversible renal endpoints provides strong clinical reassurance, supporting the continued, appropriate use of rosuvastatin in patients with varying degrees of kidney function rather than avoiding it based on theoretical concerns.¹ While rosuvastatin was associated with a higher incidence of new‑onset albuminuria, this signal was distinctly dose‑dependent, providing crucial context for its clinical management.¹ Rather than inherently indicating progressive, irreversible renal injury, this finding underscores the necessity for thoughtful dose selection, particularly for patients with advanced CKD or multiple comorbidities.¹ Importantly, this albuminuria signal was not accompanied by accelerated eGFR decline or an increased risk of ESKD, confirming its manageability in routine practice.¹ Routine monitoring of urinary albumin excretion enables early detection, allowing clinicians to make timely dose adjustments or introduce additional renoprotective interventions when necessary.
These balanced efficacy and safety outcomes are not derived from idealized trial conditions, but rather reflect real‑world clinical realities that are highly applicable to local management.¹ The study population was derived entirely from the Hong Kong HA electronic health record system, which manages over 90% of local patients with diabetes.¹ As a result, the patient characteristics, comorbidity profiles, laboratory monitoring frequencies, and prescribing behaviors directly mirror the everyday realities encountered by Hong Kong clinicians.¹ Furthermore, the study design reflects real‑world statin use by dynamically accounting for real‑world treatment patterns and long‑term follow‑up, rather than relying on static clinical trial conditions.¹ The results of this study offer insight into the safety profiles of rosuvastatin in the local setting, showing that careful monitoring should be used to achieve the favorable CV outcomes.1
Conclusion
These findings support rosuvastatin as a strong and pragmatic statin option for CV risk reduction in Hong Kong patients with diabetes, including those with CKD.¹ With appropriate dosing and routine renal monitoring, rosuvastatin offers a favorable balance between CV efficacy and renal safety.¹ The results encourage clinicians to focus on individualized statin selection and monitoring, rather than broad avoidance strategies, to optimize long‑term outcomes in this high‑risk population.¹

