MEETING HIGHLIGHT
Cabozantinib combinations leading the way in RCC: Transformative therapies backed by real-world success



The combination of targeted therapy and immunotherapy (IO) has emerged as a cornerstone in the management of advanced renal cell carcinoma (RCC), transitioning the field away from limited cytokine therapies.1 At the 'URO-ONCOLOGY Asia 2026', organized by the Hong Kong Society of Uro-Oncology, Dr. Su, Po-Jung from Chang Gung Memorial Hospital shared his insights on the holistic management of RCC. Notably, the lecture underscored the pivotal CheckMate 9ER study, which established the efficacy of the cabozantinib + nivolumab regimen, demonstrating sustained survival benefits and high response rates after five years of follow-up.2 Moreover, Dr. Su presented real-world evidence from Taiwan, bridging the gap between clinical trials and daily practice to support the regimen’s efficacy in relevant patient cohorts.3 Two cases were shared to illustrate the regimen’s potential to achieve disease-free status even in high-risk scenarios. These clinical milestones and real-world experiences have solidified the role of cabozantinib-based combinations in the evolving management of RCC, highlighting the critical integration of biological rationales and risk stratification in treating this complex malignancy.
The biological rationale: Stratifying RCC patients for cabozantinib
While localized clear cell renal cell carcinoma (ccRCC) can often be cured through surgery, metastatic disease has historically been associated with a poor prognosis.1,4 Traditional therapies primarily focused on blocking the vascular endothelial growth factor (VEGF) pathway.1 However, tumors tend to develop resistance by activating alternative “escape” pathways.4 Cabozantinib addresses this challenge through its distinctive multi-kinase inhibition profile.4 Unlike inhibitors that only target VEGF receptors, cabozantinib is a multi-tyrosine kinase inhibitor (TKI) that targets vascular endothelial growth factor receptor 2 (VEGFR2), mesenchymal-epithelial transition factor (c-MET), and AXL receptors.4 Its ability to target multiple pathways simultaneously makes it effective even after initial therapies fail.5
Dr. Su claims that although cabozantinib in combination with nivolumab provides a biological safety net for both aggressive clear cell and non-clear cell subtypes, the benefits of cabozantinib are best realized when guided by precise patient categorization, aligning the biological advantages of the therapy with the clinical needs of individual patients. Personalized care in advanced RCC starts with rigorous risk assessment, and Dr. Su emphasized the importance of the International Metastatic RCC Database Consortium (IMDC) criteria, also known as the Heng criteria, as the current gold standard for clinical decision-making. Patients are evaluated based on baseline risk factors and clinical laboratory markers, including hemoglobin levels below the lower limit of normal, and elevated corrected calcium, absolute neutrophil, and platelet counts.6 By aggregating these factors, clinicians categorize patients into favorable (0 factors), intermediate (1-2 factors), or poor (≥3 factors) risk groups.6 This stratification serves a dual purpose: it offers prognostic insights and acts as a roadmap for treatment selection.6
Current international guidelines from the European Society for Medical Oncology (ESMO) and the European Association of Urology (EAU) endorse IO-based combinations for RCC, reflecting a strong preference for these approaches.7,8 For patients at favorable risk, IO-TKI combinations, such as cabozantinib + nivolumab, are prioritized over sunitinib.7,8
CheckMate 9ER: Landmark evidence for cabozantinib + nivolumab in advanced RCC
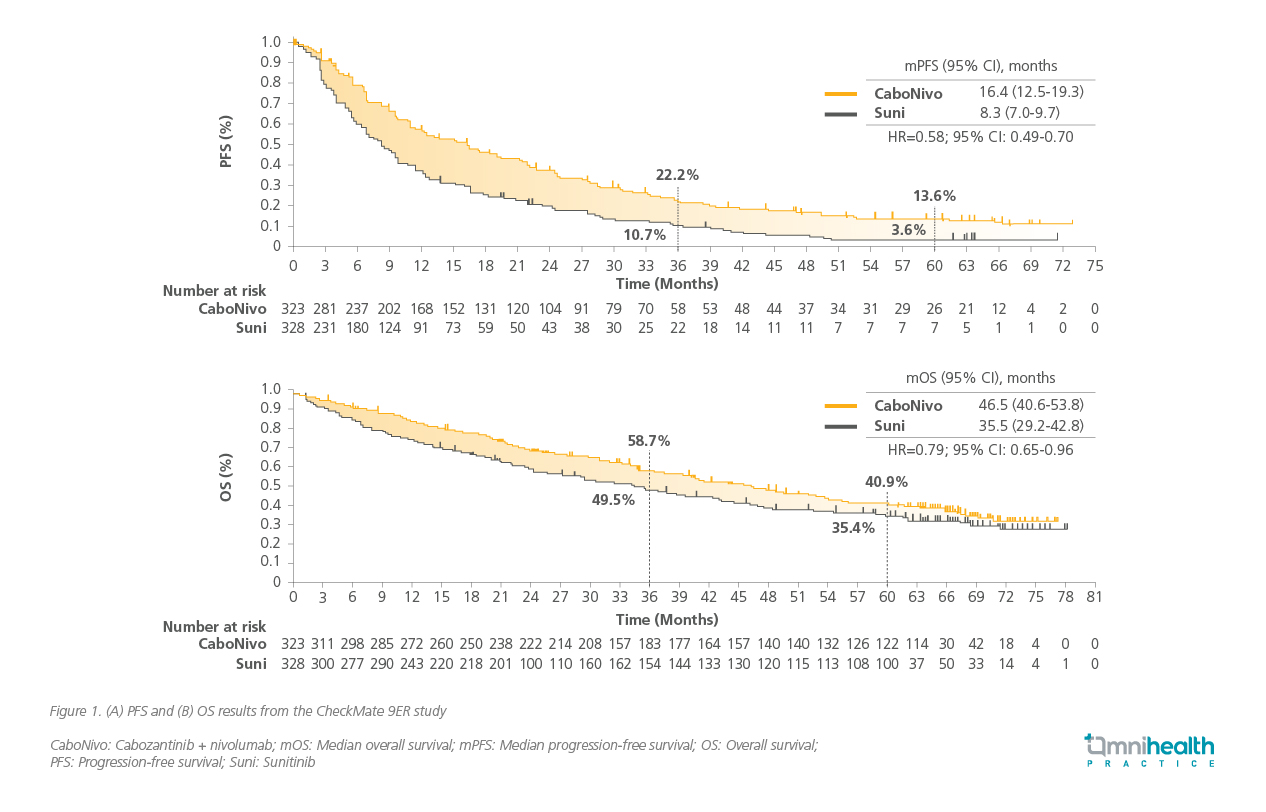
The phase 3 CheckMate 9ER trial serves as the primary source of clinical evidence, randomizing 651 patients with treatment-naïve advanced or metastatic RCC to receive either cabozantinib + nivolumab or the standard of care, sunitinib.5 With a median follow-up of 67.6 months, the results demonstrated sustained superiority of the combination over sunitinib across key endpoints.2 Cabozantinib + nivolumab achieved a median PFS (mPFS) of 16.4 months, nearly doubling the 8.3 months observed with sunitinib (figure 1A).2 The median overall survival (mOS) for the combination reached 46.5 months compared to 35.5 months for sunitinib (figure 1B), offering a 21% reduction in the risk of death (HR=0.79; 95% CI: 0.65-0.96).2 Regarding response quality, the objective response rate (ORR) was 55.7% for cabozantinib + nivolumab vs. 27.4% with sunitinib.2 The complete response (CR) rate nearly tripled to 13.9% (vs. 4.6% for sunitinib), while the rate of progressive disease (PD) was halved to 6.5%(vs. 14.3% in the sunitinib arm).2 CheckMate 9ER data showed that the combination maintained superior health-related quality of life (HRQoL) across different measures (e.g., FKSI-19, FKSI-DRS, EQ-5D-3L Index, and EQ-5D-3L VAS) and cut-offs over sunitinib, supporting Dr. Su’s emphasis that “We not only make the patient live longer, we also make them live better.”9
The safety profile for the cabozantinib + nivolumab combination remains manageable and consistent with earlier reports.2 Regarding the safety profile, discontinuations due to treatment-related adverse events (TRAEs) were 28.1% for the combination vs. 10.9% for sunitinib.2 Notably, only 10.0% of patients discontinued cabozantinib specifically due to toxicity when used in combination.2 The most frequently reported TRAEs of any grade included diarrhea, palmar-plantar erythrodysesthesia, hypothyroidism, hypertension, and fatigue.2 Beyond the overall population, subgroup analyses confirmed that efficacy was maintained even in patients with high-risk metastatic sites.2
CheckMate 9ER: Efficacy across high-risk metastatic sites
A key focus of the study was the efficacy of cabozantinib + nivolumab in patients with high-risk metastatic sites.2 Mechanistically, cabozantinib targets c-MET, a receptor tyrosine kinase frequently overexpressed in bone metastases that drives both tumor growth and bone destruction.4,10 In the CheckMate 9ER trial, patients with bone metastases showed a 57% risk reduction in progression or death (HR=0.43; 95% CI: 0.30-0.64) and a 34% risk reduction in death (HR=0.66; 95% CI: 0.45-0.95), indicating a profound benefit.2 Patients with liver metastases also showed improved outcomes on cabozantinib + nivolumab, with a 45% risk reduction in progression or death (HR=0.55; 95% CI: 0.37-0.82) and a 35% risk reduction in death (HR=0.65; 95% CI: 0.43-0.97).2 The combination remained effective for those with lung-only metastases, having shown to achieve a PFS hazard ratio of (HR=0.56; 95% CI: 0.46-0.69).2
Validating efficacy: Real-world evidence from Taiwanese patients
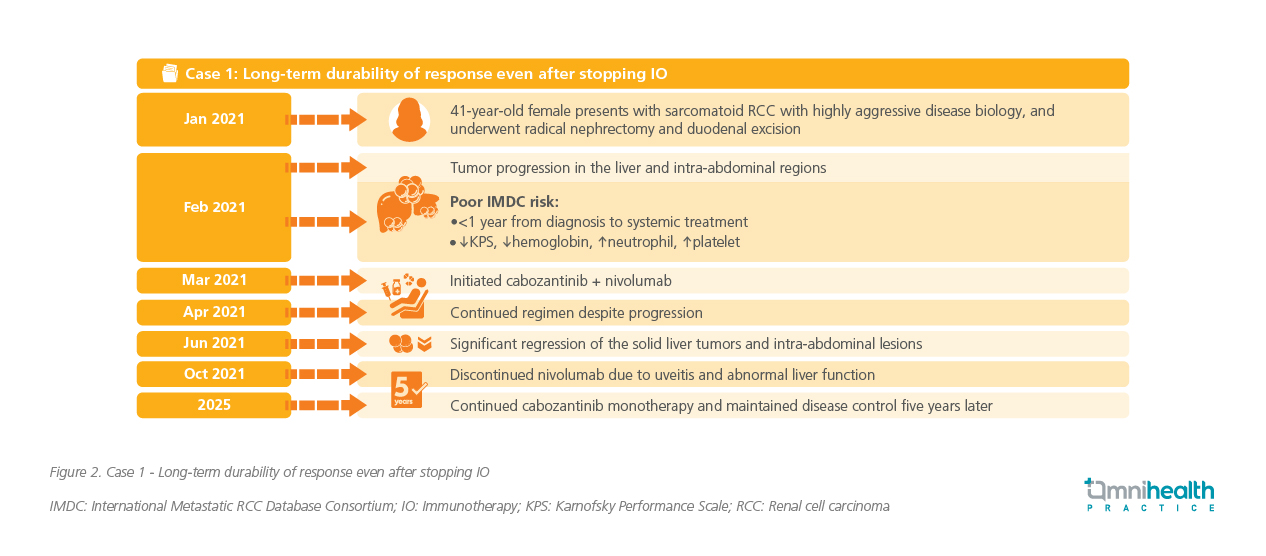
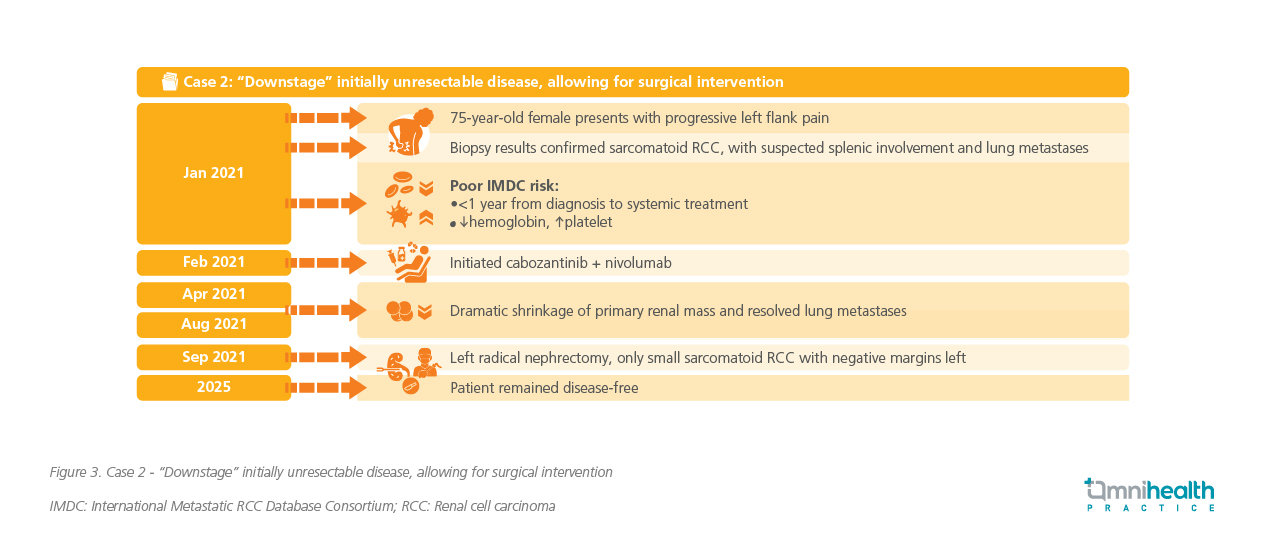
To bridge the gap between global clinical trials and clinical practice, Dr. Su presented real-world data derived from a multicentric cohort analysis, including patients from CGMH.3 This real-world study focused on a cohort of 41 Taiwanese patients treated with cabozantinib + nivolumab, evaluating whether international trial results could be replicated in a Taiwanese setting.3 Regarding response rates, the combination achieved an ORR of 52.2% in this Taiwanese cohort, closely mirroring the global CheckMate 9ER data.3 Dr. Su noted the significance of these findings: “The results are highly consistent with the pivotal study, showing both great survival benefit and a high response rate.” In terms of survival outcomes, the mPFS for the combination was not reached at the time of data cutoff, significantly outperforming the 6.3 months observed with cabozantinib monotherapy in the same dataset.3 Similarly, the mOS for the combination was not reached,” standing in stark contrast to the 11.4 months observed in the monotherapy group.3 Dr. Su supplemented these statistics with specific case examples (figure 2 & 3), affirming that the high efficacy observed in global pivotal trials is robust and replicable within the specific context of Taiwanese oncology.
Conclusion
The holistic management of RCC is no longer a “one-size-fits-all” endeavor.4 These robust clinical trial outcomes, characterized by sustained survival benefits and manageable safety profiles, provide the scientific validation for the personalized treatment strategies currently transforming patient care.2 By integrating the multi-pathway inhibition of agents like cabozantinib with the durable power of nivolumab, clinicians can achieve unprecedented survival gains.2 This comprehensive body of evidence—from global landmark trials to real-world success—underscores a paradigm shift where cabozantinib combinations ultimately allow patients to live longer and better.2,9
This is an independent editorial article, published and distributed through unrestricted educational support from IPSEN Pharma (Hong Kong), for the purpose of continuing medical education only. The views expressed in this publication reflect the experience and/or opinion of the author(s) and are not necessarily those of editors, publisher and sponsor(s). Because of rapid advances in medicine, independent verification of clinical diagnoses, medical suitability and dosage should be made before treatment prescription. The appearance of advertisement, if any, has no influence on editorial content or presentation and does not imply the endorsement of products by the publication, or its authors and editors.
- Ozay ZI, et al. Treatment and Attrition Trends for Metastatic Clear Cell Renal Cell Carcinoma in the US. JAMA Netw Open. 2025;8(3):e251201.
- Motzer RJ, et al. Final analysis of nivolumab plus cabozantinib for advanced renal cell carcinoma from the randomized phase III CheckMate 9ER trial. Ann Oncol. 2026;37(1):33-43.
- Ku CH, et al. Cabozantinib versus cabozantinib plus nivolumab in first-line treatment of advanced renal cell carcinoma: A Chang Gung Medical Foundation multicentric cohort, real-world study. [303P] presented at ESMO Asia Congress 2024; Singapore; 6-8 Dec 2024.
- Hashmi MF, et al. Renal clear cell cancer. StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/NBK563230/. Accessed March 12, 2026.
- Choueiri TK, et al. Nivolumab plus Cabozantinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. 2021;384(9):829-841
- Heng DY, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol. 2009;27(34):5794-9.
- Bex A, et al. European Association of Urology Guidelines on Renal Cell Carcinoma. EAU Guidelines Office, Arnhem, The Netherlands. Available at: http://uroweb.org/guidelines/compilations-of-all-guidelines/. Accessed March 12, 2026.
- Powles T, et al. Renal cell carcinoma: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2024;35(8):692-706.
- Cella D, et al. Patient-reported outcomes with first-line nivolumab plus cabozantinib versus sunitinib in patients with advanced renal cell carcinoma treated in CheckMate 9ER: an open-label, randomised, phase 3 trial. Lancet Oncol. 2022;23(2):292-303.
- Silva Paiva R, et al. c-Met expression in renal cell carcinoma with bone metastases. J Bone Oncol. 2020;25:100315.

