MEETING HIGHLIGHT
Optimizing bipolar disorder treatment with antipsychotics and long-acting injectables



Globally, the use of antipsychotic (AP) long-acting injectables (LAIs) in bipolar disorder (BD) is becoming increasingly common.1 In a recent seminar, Dr. Lin, Shih-Ku, from the Taipei Chang Gung Memorial Hospital, shared the recent trends of increasing AP utilization.1 He also shared real-world evidence (RWE) demonstrating the efficacy of LAIs in preventing relapse and reducing healthcare costs across diverse populations.2,3 Despite these benefits, regional prescribing patterns—such as the notably low usage rates in Hong Kong highlighted by the REAP study—remain a concern.4 In another seminar, Dr. Fang, Chun-Kai, from the MacKay Memorial Hospital in Taiwan, emphasized the critical role of shared decision-making (SDM) to overcome stigma and align clinical practice with the latest international guidelines and consensus recommendations to achieve proper utilization of LAI.5-7
The paradigm shift to APs and LAIs
Characterized by recurrent mood oscillations and instability, BD is a chronic clinical condition affecting 1%-2% of the general population.² Beyond its core symptoms, BD is associated with severe consequences, including poor quality of life, co-occurring addiction and physical illness, and high mortality.² Relapses into depressive or manic states frequently necessitate increased utilization of mental health services and are often directly attributable to poor treatment adherence.² Dr. Lin described that while pharmacotherapy for BD was traditionally anchored by mood stabilizers like lithium, modern polypharmacy increasingly relies on APs to achieve broad-spectrum mood stabilization. However, adherence remains one of the greatest predictors of long-term outcome; high rates of treatment discontinuation directly fuel the cycle of relapse and re-hospitalization.³
Atypical APs provide proven efficacy across the entire BD spectrum.6 Recognizing the limitations of relying solely on oral medications, particularly concerning patient compliance, the clinical focus has broadened.² LAIs represent the next evolution, offering a critical, proactive intervention to ensure consistent drug concentrations and address non-adherence, thereby optimizing long-term outcomes.4 Dr. Lin reminded that “Clinicians must actively challenge the ingrained perception that LAIs are solely a treatment of last resort, embracing their potential for early, sustained intervention.”
Prescription patterns in Hong Kong vs. Asia
The Research on Asian Prescription Patterns for Bipolar Disorder (REAP-BD) study provides a crucial regional context, particularly for BD management in Asia.4 The cohort had high reliance on APs, with around 82.1% of patients receiving AP medication.¹ However, the utilization of the LAI formulation starkly contrasts with this high general AP usage.4 Across the entire REAP-BD consortium, the average LAI utilization rate was low at 5.1%.4 The LAI use percentage in Hong Kong was found to be particularly low at 3.3% (1 out of 30 patients).4 This discrepancy—where high overall AP prescription meets low LAI adoption—points unequivocally to non-clinical systemic and perceptual barriers that need to be addressed to improve patient care in Hong Kong.8
Increasing use and favorable outcomes of APs and LAIs in BD
Over the last two decades, clinical practice has decisively shifted.9 AP prescriptions for bipolar outpatient visits increased significantly from 12.4% in 1997-2000 to 51.4% in 2013-2016 in the United States, illustrating that second-generation APs have largely supplanted traditional mood stabilizers as monotherapy or adjunctive treatment.9 Dr. Lin reflected that “the shift in prescribing patterns reflects their established efficacy and generally manageable side-effect profiles compared to first-generation agents. The need for APs underscores that BD is often a complex condition requiring polypharmacy or combination treatments to achieve and maintain stability.”
The inherent benefit of LAIs is quantified through mirror-image studies, which compare a patient's outcomes before and after LAI initiation.² Data from these studies have demonstrated that LAI treatment initiation is associated with a statistically significant decrease in the frequency of mood episodes and hospitalizations.² Large-scale, register-based national cohort studies also found LAIs to be associated with lower psychiatric admission risks compared to oral APs in patients with BD.10 Across a general BD population, LAIs were associated with a 28% lower risk of psychiatric admission than their oral counterparts.10 Importantly, the superiority of LAIs was also evident in first-episode patients.10
Dr. Lin highlighted that another clinical advantage of LAIs is their pharmacokinetic profile upon cessation. He claimed that “The long half-life of LAI formulations results in a substantial delay in time to recurrence compared to the immediate loss of protection seen upon discontinuation of an oral equivalent.” This extended therapeutic buffer provides a critical window for intervention and relapse prevention, further supportive of their proactive use.
Clinical outcomes of AP and LAI use
While real-world data consistently validates the effectiveness of LAIs at a population level, rigorous clinical trials are necessary to demonstrate the safety and sustained efficacy of individual agents. A study evaluated aripiprazole once-monthly 400mg (AOM 400) as a maintenance treatment for patients with Bipolar I Disorder (BP-I), enrolling both AOM 400-naive and AOM 400-experienced patients from a randomized placebo-controlled trial.11 The treatment demonstrated strong effectiveness over the 52-week open-label phase, with the vast majority of patients maintaining stability.11 97.6% of rollover patients (those already experienced with AOM 400) maintained stability through their last visit.11 87.0% of de novo patients (new to AOM 400) also maintained stability through their last visit.11 The overall requirement for rescue medication (e.g., lithium or valproate) to manage instability was very low, involving less than 10% of the total patient cohort.11
The overall discontinuation rate due to treatment-emergent adverse events (TEAEs) was contained at 10.1%.11 The most commonly reported TEAEs (occurring in ≥5% of patients) included akathisia (up to 15.8% in de novo) and weight increase (up to 14.8% in de novo).11 TEAEs were generally more common in the de novo group than the rollover group, suggesting that initial tolerability issues tend to resolve or are successfully managed as treatment continues.11
Patients reported high levels of satisfaction with AOM 400, indicating strong acceptability for a long-term treatment.11 Most patients perceived AOM 400 to have a favorable side effect profile compared to their previous medications.11 Over 66% of de novo patients and nearly 73% of rollover patients reported experiencing “no side effects“ or “much less side effects“ on AOM 400 compared to previous treatments.11 Efficacy, as measured by mean changes in YMRS (Young Mania Rating Scale) and CGI-BP-S (Clinical Global Impressions-Bipolar-Severity of Illness) scores, was successfully maintained throughout the 52 weeks, confirming AOM 400's efficacy as a long-term mood stabilizer.11
Current consensus and guidelines on LAI use
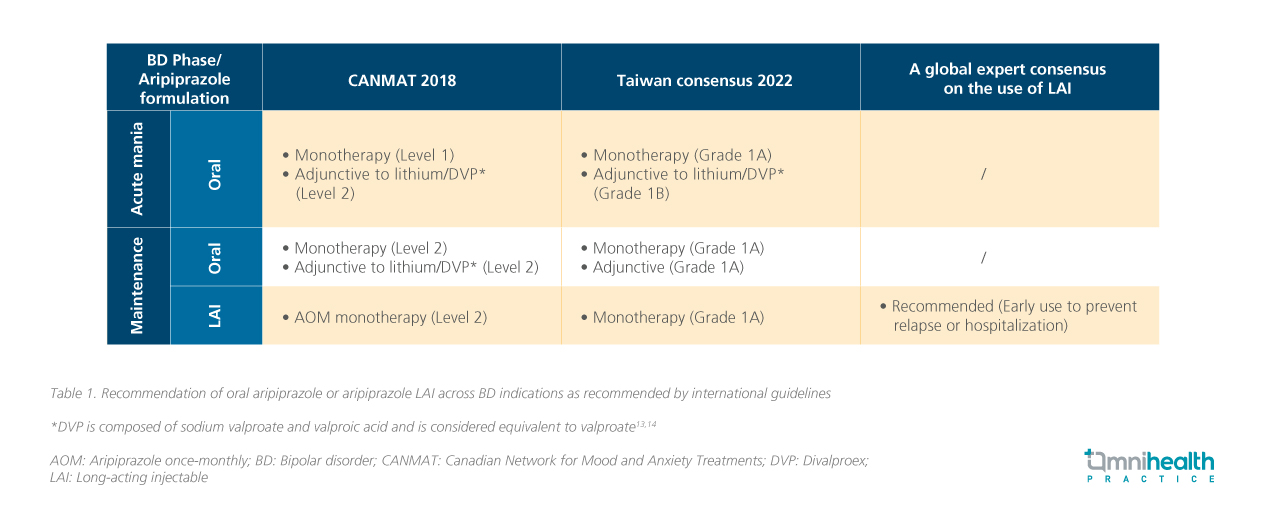
Given the clinical and economic evidence demonstrating the efficacy of LAIs in preventing relapse and ensuring stability, major regional and international psychiatric bodies have integrated these findings into official consensus and treatment guidelines. The 2022 Taiwan consensus on BD treatment provides a clear, evidence-based direction.12 Oral aripiprazole for the acute manic phase is designated with a grade 1 (strong) recommendation.12 Crucially, the maintenance phase recommendations also reflect strong support for the LAI formulation.12 This grade 1 recommendation places LAI aripiprazole on the highest tier (grade 1A) of approved maintenance treatments, reinforcing its role as a gold-standard option.12
International guidelines further substantiate this proactive approach (table 1).6,7,12 The latest Canadian Network for Mood and Anxiety Treatments (CANMAT) and the International Society for Bipolar Disorders (ISBD) guidelines explicitly list AOM as a first-line treatment for maintenance therapy.6 Recognizing the universal reluctance to adopt LAIs early, a global expert consensus published in 2024 provided clear guidance.7 It stressed that LAIs are not solely for patients with the most severe disease or established sub-optimal adherence.7 Instead, they advocated for a proactive, preventive approach.7
Barriers and solutions to LAI adoption
Regarding the barriers to LAI adoption, Dr. Fang shared that the primary challenge to LAI adoption is largely perceptual, rooted in widespread cultural stigma. LAIs are often underutilized because they are culturally and clinically associated with “chronic,“ “severe,“ or “refractory“ illness. This results in misperceptions by patients (fear of needles, feeling stigmatized) and clinical deferral by prescribers, who often reserve LAIs as a punitive “last resort“ rather than a proactive, preventative tool. This late-stage intervention greatly limits the full potential of LAIs to protect against the earliest, most damaging relapses. SDM offers an effective solution to overcome these barriers, shifting the patient-clinician dynamic from one of mandatory compliance to a therapeutic partnership. The SDM philosophy moves fundamentally from a compliance model or simple “informed consent“ to “shared participation,“ requiring the clinician to integrate patient preferences, values, and concerns alongside the best clinical evidence. SDM relies on structured communication models, such as the Three-Talk Model. This model consists of three stages: “Team Talk,“ which establishes a partnership between clinician and patient; “Option Talk,“ where treatment options are presented neutrally; and “Decision Talk,“ in which the final choice is made based on the patient's values.15 These models utilize educational and interactive tools to achieve several key purposes. Dr. Fang expressed that, first, they combat stigma by reframing LAIs as proactive, high-efficacy treatment options through psychoeducation. Second, they elicit patient values using worksheets to clarify concerns, such as fear of needles, and preferences for treatment. Finally, they ensure transparency by providing side-by-side comparison tables of LAIs and oral medications, enabling informed patient choices.
Dr. Fang reiterated that Taiwan's successful blueprint for SDM adoption has demonstrated that by empowering patients and engaging all stakeholders, it is possible to significantly increase the acceptance of LAI treatment. This model was encouraged to be localized, focusing on tailoring the conversation to cultural nuances and emphasizing the long-term benefits and cost-effectiveness of LAIs to clinicians and patients in regions like Hong Kong.
Conclusion
The clinical evidence for the use of LAI in BD indicates promising outcomes in reducing hospitalization, and preventing relapse.2,10 This is recognized by international bodies that place LAI aripiprazole on the recommended list. Both Dr. Lin and Dr. Fang reminded that the path forward demands a fundamental change in mindset: LAIs should be offered proactively as an early, efficacious option, not a reluctant “last resort.“ This change may be driven by the widespread adoption of SDM, which empowers patients, neutralizes stigma, and ensures that clinical decisions truly reflect the best available evidence and the patient’s informed preferences.

