Highlights
- Functional dyspepsia (FD) is challenging to treat due to its complex biopsychosocial pathophysiology
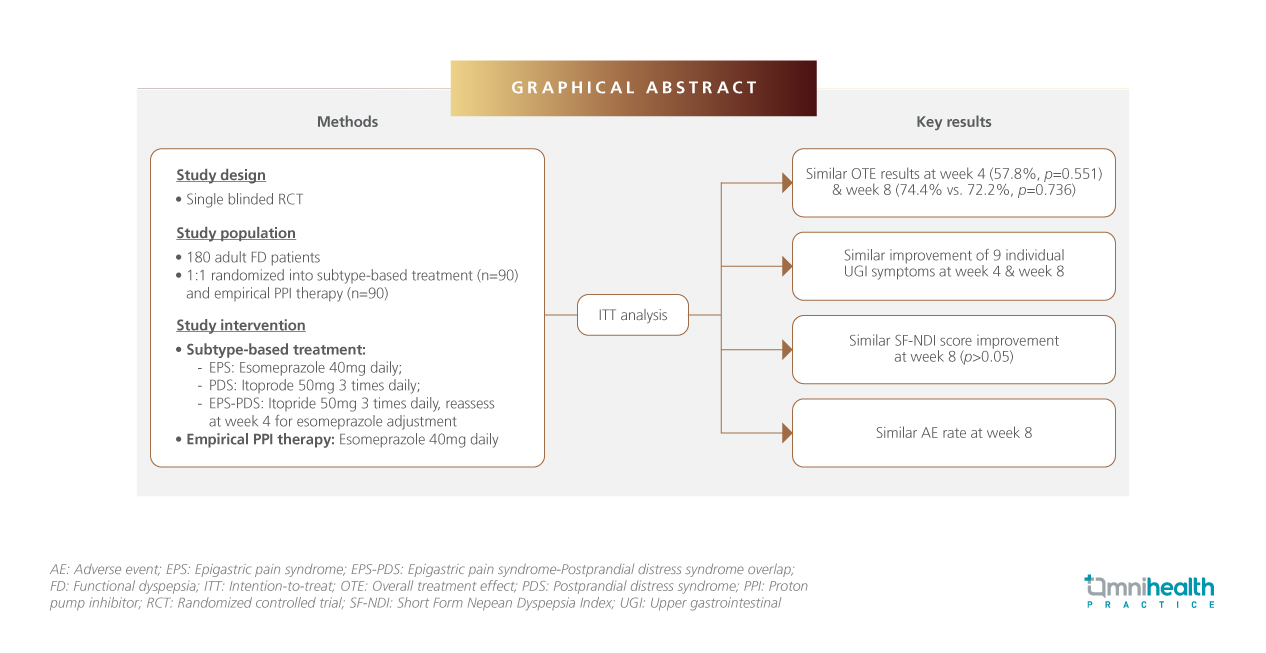
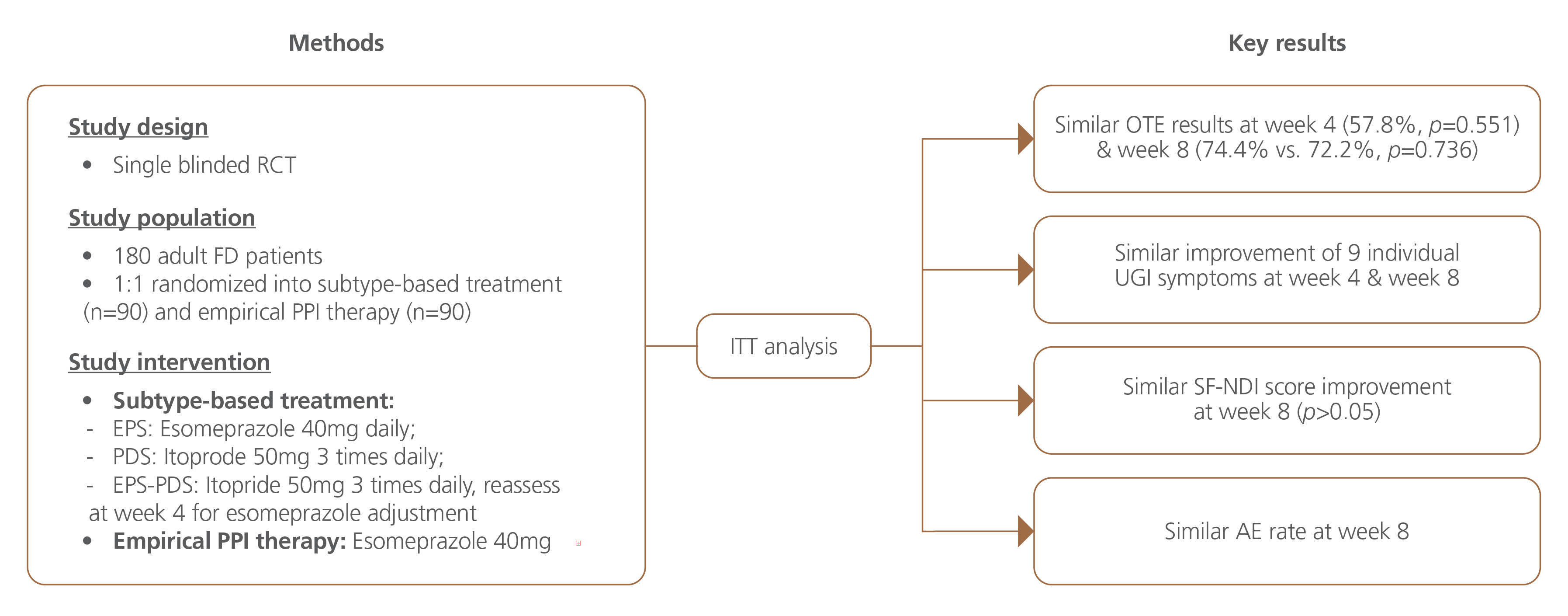
- Given the conflicting recommendations for initial therapy, a single-blinded, randomized controlled trial (RCT) was conducted to compare the efficacy of subtype-specific treatment with empirical proton pump inhibitor (PPI) therapy
- The findings suggest that subtype-based treatment is comparable to empirical PPI therapy as an initial approach. Both treatment strategies appear to be safe, with a similar rate of adverse events (AEs)
- Dr. Chuah, Kee-Huat, the lead author of this study, presents prokinetics as a promising, evidence-based alternative for patients with postprandial distress syndrome (PDS) subtype
![]()
![]()
AE: Adverse event; EPS: Epigastric pain syndrome; EPS-PDS: Epigastric pain syndrome-Postprandial distress syndrome overlap; OTE: Overall treatment effect; PDS: Postprandial distress syndrome; PPI: Proton pump inhibitor; SF-NDI: Short Form Nepean Dyspepsia Index
In brief
Functional dyspepsia (FD) is a common gut-brain interaction disorder that primarily affects adults and imposes a significant economic burden.1 Treatment guidelines vary, leading to inconsistencies in management approaches.1 A randomized, single-blinded trial was conducted to evaluate the efficacy of subtype-specific treatment vs. empirical proton pump inhibitor (PPI) therapy in adults with FD.1 Findings suggest that both treatment approaches significantly improved the overall symptoms and health-related quality of life (HRQoL), with no clear advantage of either, over another in FD management.1
Background
FD is a highly prevalent disorder of gut-brain interaction (DGBI), commonly affecting adults.1 It is characterized by persistent upper gastrointestinal (UGI) symptoms such as early satiety, postprandial fullness, epigastric burning, and epigastric pain without an identifiable cause following clinical assessment.1 FD is further classified into two subtypes: epigastric pain syndrome (EPS) and postprandial distress syndrome (PDS).1 Although not life-threatening, FD significantly impacts HRQoL due to persistent symptoms and associated psychological distress.1
The complex biopsychosocial nature of FD presents challenges in treatment.1 Current pharmacological options primarily include PPIs and prokinetics.1 PPIs are thought to alleviate symptoms by improving duodenal permeability, reducing microinflammation, and enhancing acid clearance, while prokinetics enhance gastric motility and accommodation.1 However, treatment recommendations vary across guidelines.1 The American College of Gastroenterology and the Canadian Association of Gastroenterology advocate for PPI therapy as the first-line treatment for all FD patients, irrespective of subtype.2 In contrast, both the Asian and Rome consensus reports suggest a subtype-based approach, recommending prokinetics (e.g. itopride) for PDS, and PPIs for EPS.3,4 Meanwhile, the British Society of Gastroenterology guidelines acknowledge the efficacy of both PPIs and certain prokinetics, but do not specify a preferred treatment for EPS or PDS due to insufficient evidence.5
Given these conflicting recommendations, a randomized controlled trial (RCT) was conducted to evaluate the efficacy of subtype-specific treatment compared to empirical PPI therapy as an initial approach for FD.1
Methodology
This study was a randomized, single-blinded interventional trial comparing subtype-specific treatment vs. empirical PPI therapy over an 8-week period in adult patients with FD.1 The study population included adults diagnosed with FD according to the Rome IV criteria.1 EPS was defined as epigastric pain or burning occurring at least once a week, while PDS was characterized by bothersome post-meal abdominal discomfort or fullness at least three times a week.1 To be eligible for inclusion, symptoms had to have persisted for at least three months before recruitment, with onset at least six months prior to diagnosis.1 Patients who were pregnant or with overlapping irritable bowel syndrome, severe anxiety or depression, active Helicobacter pylori infection, or any confirmed organic cause for gastrointestinal symptoms were excluded.1 Participants previously using PPIs or itopride underwent a 14-day washout period before enrolment.1
The subtype-specific treatment group received therapy based on FD subtype: EPS was treated with esomeprazole 40mg daily, PDS with itopride 50mg three times daily, and EPS-PDS overlap with itopride 50mg three times daily, with reassessment at week 4 to determine whether esomeprazole should be added or substituted.1 The empirical therapy group received esomeprazole 40mg daily, regardless of subtype.1 Both groups underwent an 8-week treatment period.1 The primary outcome was symptom improvement, measured using the ‘Overall Treatment Effect’ (OTE) questionnaire on a 7-point Likert scale.1 Secondary outcomes included changes in UGI symptom severity, HRQoL assessed via the Short Form Nepean Dyspepsia Index (SF-NDI), and adverse events (AEs).1
A total of 229 patients were screened, with 180 meeting eligibility criteria and randomized 1:1 using a computer-generated sequence, into the subtype-specific treatment group (n=90) and empirical treatment group (n=90) for an intention-to-treat (ITT) analysis.1 The median age of participants was 50 years, and 68.7% were female.1 The most common FD subtype was PDS (56.7%), followed by EPS-PDS overlap (32.8%), EPS (10.6%), and 14.4% having FD-gastroesophageal reflux disease (FD-GERD) overlap.1 The median body mass index (BMI) was 23.6kg/m2 (range: 21.1kg/m2-26.9kg/m2).1
Results
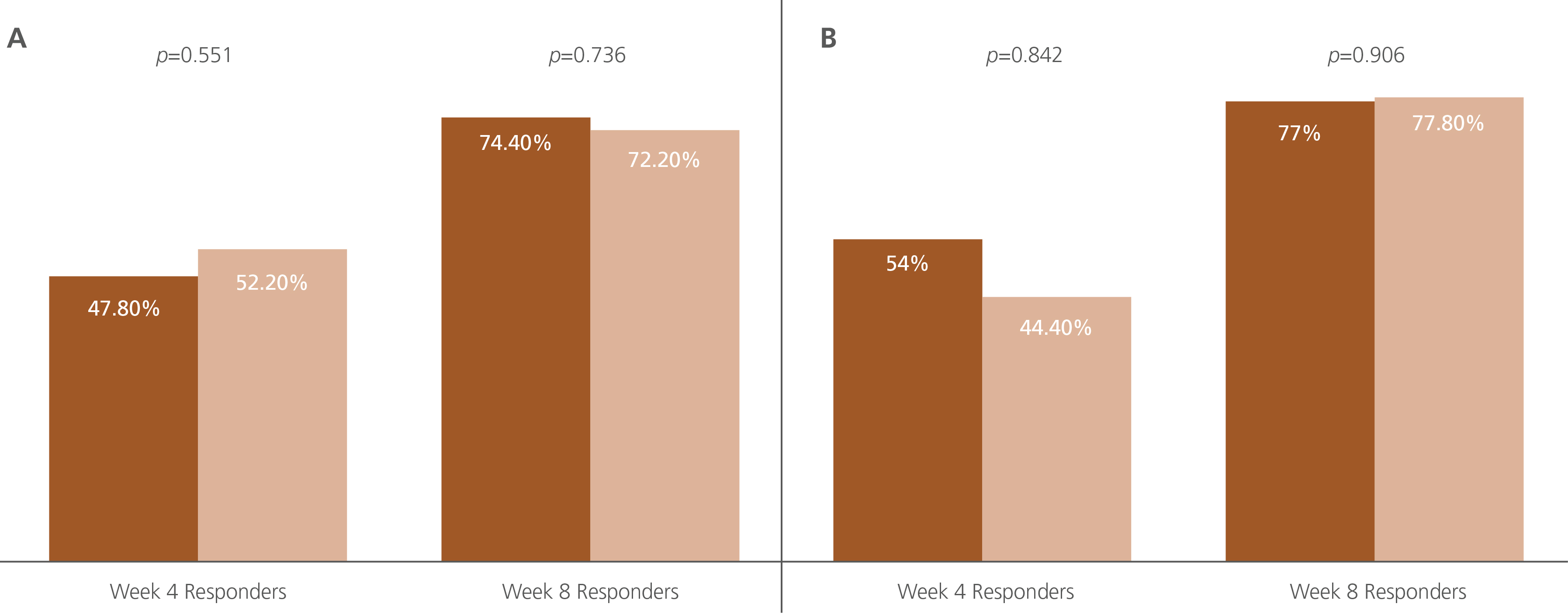
At week 8, the overall response rate based on the OTE questionnaire was similar between the subtype-specific treatment and empirical treatment groups (74.4% vs. 72.2%, p=0.736) (figure 1).1 Both groups also showed similar improvements in individual UGI symptoms (table 1).1
![]()
|
|
Subtype-specific therapy group
|
|
|
Empirical therapy group
|
Figure 1. OTE at week 4 and week 8 for the intervention and control groups in the (A) intention-to-treat analysis and (B) per protocol analysis
![]()
Table 1. UGI symptoms improved by 50% in intervention and control groups
CI: Confidence interval; UGI: Upper gastrointestinal
While HRQoL was significantly improved (p<0.001), the overall SF-NDI score changes remained comparable between groups (p>0.05).1 However, AEs were significantly more frequent in the empirical therapy group at week 4 (35.6% vs. 18.9%, p=0.012), though the difference diminished by week 8.1 The most common AEs in the subtype-specific therapy group were diarrhea, nausea, and dizziness at week 4, followed by increased hunger, constipation, and diarrhea at week 8.1 In the empirical therapy group, diarrhea, increased hunger, and flatulence were the most frequently reported AEs at both weeks 4 and 8.1
Among patients with EPS-PDS overlap in the subtype-specific therapy group (n=59), 25.9% required the addition of a PPI, while 14.8% were non-responders and needed to switch to PPI treatment at week 4.1 Treatment adherence was slightly lower in the subtype-specific therapy group at week 4 (94.2% vs. 97.3%, p=0.032) but became comparable between groups by week 8 (92.1% vs. 94.7%, p=0.112).1
Discussion
In an exclusive interview with Omnihealth Practice, Dr. Chuah, Kee Huat explained the significance of their findings: prokinetics offer a viable, comparable alternative for patients with PDS subtype or PDS overlap. Designed as a head-to-head comparison between subtype-specific treatment and empirical PPI therapy, the study aimed to bridge gaps in current clinical guidelines, which provide inconsistent recommendations for FD management. This evidence is particularly relevant as physicians often prescribe PPIs for FD, despite growing concerns over their long-term use.
“It is well-documented that PPIs are widely prescribed, and literature suggests that prolonged use has been linked to complications such as Clostridium difficile infections, aspiration pneumonia, small intestinal bacterial overgrowth (SIBO), nutrients malabsorption, and osteoporosis, among others,” Dr. Chuah explained. “This study aims to provide an evidence-based alternative, highlighting the clinical value of distinguishing between the two primary FD subtypes—PDS and EPS. This distinction enables more tailored treatment strategies, including switching to prokinetics for PDS patients rather than relying solely on PPIs,” he elaborated. While he acknowledged that tapering off PPIs can be challenging for patients with persistent symptoms, as patients often develop psychological dependence, Dr. Chuah emphasized the importance of gradually reducing PPI use or maintaining the lowest effective dose of PPI whenever possible. When asked about treatment options beyond PPIs and prokinetics, Dr. Chuah highlighted that neuromodulators, such as amitriptyline, may be beneficial—particularly for patients with concomitant insomnia, mild anxiety, or diarrhea.
Dr. Chuah also mentioned the intricate pathophysiology of FD as a potential factor influencing the study findings. The underlying pathophysiological mechanisms driving FD symptoms—such as visceral hypersensitivity, impaired gastric accommodation, duodenal microinflammation, and duodenal acid exposure may be interconnected and occur with similar prevalence across patients with EPS, PDS, and those with EPS-PDS overlap. This challenges the conventional notion that each FD subtype exhibits more homogenous pathophysiology, highlighting the difficulty in predicting treatment responses. Given FD’s multifaceted nature, he also stressed the importance of identifying overlapping conditions, including other DGBI, functional gastrointestinal disorders (FGID), GERD, and psychiatric comorbidities. Addressing these factors, he noted, is crucial for improving treatment outcomes, as FD often has a bidirectional relationship with other conditions.
A key limitation of this study, as highlighted in the paper, is its potential lack of statistical power, as the sample size was calculated based on an earlier study estimating a 24% difference in symptom improvement between PPI and prokinetic treatments.1 However, a subsequent network meta-analysis, published after the study's initiation, reported a smaller difference, suggesting that the originally planned sample size may have been insufficient to detect a true effect, and the findings should be considered preliminary.1
Furthermore, given the substantial healthcare burden of FD, Dr. Chuah referenced his previous research, noting that FD accounts for 36.7% of FGID cases in secondary care gastroenterology clinics, with the highest resource utilization.6 Dr. Chuah shared key perspectives in managing FD, emphasizing that it should be a positive diagnosis grounded in the Rome IV criteria. He underscored the necessity of more sinister diagnoses, such as malignancies, by carefully evaluating red-flag symptoms. While subclassifying FD into distinct subtypes can help guide treatment decisions, he stressed that identifying and addressing comorbidities associated with FD is equally crucial for optimizing patient outcomes. Building on these findings, efforts are focused on establishing an evidence-based foundation for refining clinical guidelines, leveraging insights gained from clinical trials to improve patient care and FD treatment strategies.
Conclusion
In conclusion, this study suggests that treating FD based on subtype appears to be non-inferior to empirical PPI therapy as an initial strategy, with both approaches demonstrating safety and similar rates of adverse events.1 These findings underscore the potential clinical value of a more tailored approach that aligns treatment with FD subtype rather than defaulting to empirical PPI use. However, given the potential limitations of sample size and statistical power, larger-scale trials are needed to validate these results, refine treatment algorithms, and establish a more standardized, evidence-based framework for FD management.1
“Prokinetics offer a viable, comparable alternative for patients with PDS subtype or PDS overlap”
Dr. Chuah, Kee-Huat
Associate Professor,
Consultant Gastroenterologist & Hepatologist,
Faculty of Medicine, University of Malaya,
Kuala Lumpur, Malaysia